News & Blogs
Why she was involved in the dysphagia diet
How we eat and how we swallow food
Importance of oral food intake
The dysphagia pyramid
In this blog, we touch on diverse topics about Japanese food cultures, practices together with the culinary secret, TREHA®, and its important role in the Japanese food industry. We hope our blog helps you obtain in-depth knowledge of the secrets and science behind Japanese cuisine, shared from our kitchen, to yours.
This blog presents an interview held in 2019 with Ms. Setsuko Kanaya, a pioneer in the development of the dysphagia diet in Japan. She has worked as head of the nutrition department at Seirei Mikatahara General Hospital, and a former professor at Hamamatsu University. In 2013, she established the ‘Kanaya Nutrition Institute’.
In developed countries, the population is aging. The United Nations define an 'aged society' as a society in which more than 14% of the population is 65 years or older. Surprisingly enough, 56 of 194 countries in the world are already within the definition. Thus, being health-conscious has been of focus in all countries, especially those with a large aging population. People exercise to develop their muscles, and try to make their diet healthy for vitality and to prevent chronic disease. However, not many people know that an indicator of aging is not only in appearance or in changes in blood tests.
Swallowing, which is the act of passing food from the mouth to the stomach, through the throat and esophagus, can change as we age. The movement, which everyone does every single day without thinking, is much more complicated than you can imagine. As with all functions of our body, as we age, swallowing function can decline. In fact, many of the elderly suffer from dysphagia (difficulty swallowing), and Japan is no exception.
One of the serious problems caused by dysphagia is pneumonia, caused by food residue in the throat after meals. Japan is a 'super-aged society' according to the United Nations’ definition, around 30% of the population is over 65 years old. Pneumonia is already one of the major causes of death in the elderly in Japan, who are super-aged and more aspiration prone. It is reported that around 80% of cause of death in the elderly over 80 years old is due to aspiration and pneumonia. To keep the elderly healthy, comprehensive efforts targeted at dysphagia has been necessary in Japan.
The dysphagia diet has already been recognized amongst Japanese, and packaged foods for dysphagia have increased in numbers on supermarket shelves, thanks to the contribution of many people, including Ms. Kanaya. It must have been an enormous challenge to develop a dysphagia diet from scratch. How did Ms. Kanaya begin to develop this diet, and what does she think about the current status of the dysphagia diet in Japan?
"Our action for developing dysphagia friendly food started from learning about ‘food boluses’."
Team TREHA®: Why and how did you start learning about dysphagia?
Ms. Kanaya: I have worked at Seirei Mikatahara General Hospital in Japan, as chief of the nutrition division. In 1980s, dementia patients have increased, and a doctor asked me if he could make the patients take an imaging agent via an oral route for an examination. Patients with dementia tend to suffer from dysphagia, which is difficulty swallowing, so I started to think about how to get them to take a large enough amount of the imaging agent without aspirating.
Team TREHA®: It’s surprising that you started thinking about liquid, rather than solid.
Ms. Kanaya: Although many people think water is the easiest material to drink, that's not true. The mechanism of swallowing is actually complicated and sensitive, and liquid without viscosity such as water and tea are relatively difficult to swallow. I wanted to make liquid easier to drink for patients that have dysphagia, but there were no precedents or reference literature in Japan. I deciphered English literature from the U.S., and learned about the importance and concept of the ‘food bolus’. A food bolus is a mass of food you swallow, formed in the mouth by chewing. Everyone makes a food bolus while eating. Making a food bolus is key for swallowing; thus, I started to think about how to make a ‘mass’ of food, regardless of its form (e.g. liquid, solid).
Processes of chewing and swallowing
Although we are not conscious of it, we repeat the 5 steps below when eating. If any steps are dysfunctional, it would be defined as dysphagia.
Judging texture, hardness and temperature of food.
Chewing food and making a food bolus.
Transferring the food bolus to the pharynges by movement of the tongue.
Transferring the food bolus from the pharynges to the esophagus by swallowing.
Transferring the food bolus to the stomach through peristaltic activity of the esophagus.
Importance of the oral food intake – Promoting both body and mental health
Team TREHA®: I’d like to ask you why you think food for those who are dysphagic is important, before asking more about your story.
Ms. Kanaya: Patients face many problems if they have dysphagia. I’d like to touch on 3 main issues for dysphagia patients below. Japan is an aging society, and I’m sure the importance of a dysphagia diet has been increasing.
Decreasing the Quality of Life
Quality of Life refers how well we live, and how fulfilled we are as a human being. Eating by mouth is not only important for keeping our body healthy, but also our mental health - by enjoying the taste and flavor of food. In addition, moving eating-related organs such as the buccal cavity, pharynges, esophagus, stomach and even a brain contributes to maintaining full capability of our functions as a human. Quality of Life is closely related to food intake - and it decreases if eating and swallowing function decreases.
Malnutrition, dehydration
Difficulty of food intake by mouth may cause malnutrition and dehydration among patients. It is said that about 40% of aging patients in Japan who are in the hospital or the nursing home suffer from malnutrition caused by dysphagia. Malnutrition leads to many health problems such as infectious diseases and slow recovery from any health issues.
Aspiration, suffocation
Aspiration is taking foreign matter, such as saliva and food, accidentally into the respiratory tract. Although a healthy person may choke to remove unwanted matter from the respiratory tract, a dysphagic patient cannot do it. Unwanted matter in the respiratory tract may cause suffocation, or inflammation by surface-associated bacteria, which leads to pneumonia.
Ms. Kanaya: The ‘dysphagia diet’ is key for preventing the issues described above, and giving the joy of eating to patients who have had dysphagia impact their lives. Seirei Mikatahara General Hospital has started to provide the dysphagia diet since 1987, and improved it by adapting the framework for a ‘step-by-step dysphagia diet’, to provide the appropriate form of food to patients. The ‘step-by-step dysphagia diet’ has developed into the ‘dysphagia pyramid’, and was officially introduced during the 10th meeting of the Japanese Society of Dysphagia Rehabilitation (JSDR) in 2004. The concept delivered during this meeting has been rolled out throughout hospitals in Japan. The concept continues to be updated; the ‘Japanese Dysphagia Diet 2013’ has been published by JSDR dysphasia diet committee, and accepted by many hospitals and nursing homes in Japan.
What is the dysphagia pyramid?
It is the standardization of food form and hardness across 6 levels. Levels are set along with difficulty of eating and swallowing. The ordinary diet is Lv.5, nursing care food is Lv.4 and the dysphagia diet is under Lv.3. Patients are served food with appropriate levels along with their ability. As dysphagia progresses, levels tend to decrease to accommodate the loss of swallowing function.
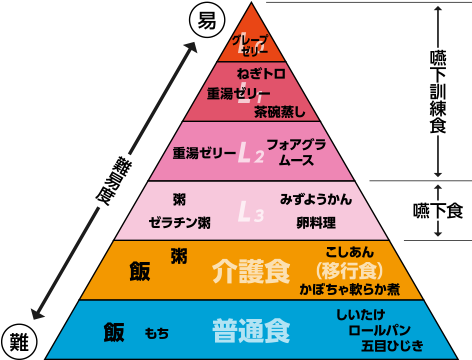
Example of food:
L0: grape jelly
L1: minced raw tuna
L2: foie gras mousse
L3: omelet
Nursing care food: simmered soft pumpkin, porridge
Ordinary diet: dinner roll, mushrooms
Cited by: engesyoku.com
IDDSI – The Global Standard
Globally, IDDSI (International Dysphagia Diet Standardization Initiative) categorizes food and beverages into 8 levels for patients. IDDSI operates to ensure ‘common language’ among dysphagia patients, caretakers, health professionals and people in the food industry.
Column: Isn’t the “finely-chopped diet” same as “dysphagia diet”?
You might imagine a 'finely-chopped diet' when you think about food for the elderly. A finely-chopped diet has often been provided to the elderly in Japan in past years, however we are beginning to understand that it is not actually suitable for them. For a finely-chopped diet, all ingredients are chopped together without thinking of the foods hardness. This tends to cause many bits and pieces to be in the mouth, making it difficult to form a food bolus for swallowing. Aspiration can occur because the food that cannot be incorporated into a food bolus remains in the pharynges. The finely-chopped diet is also not good for food safety; chopped ingredients have a larger surface, and the risk of contamination is increased. The risk of a finely-chopped diet have been recognized in Japan, and foods that are more easily incorporated into a food bolus are considered when planning meals for patients and the elderly.
On today’s blog, we showed why Ms. Kanaya started to think about dysphagia diet, the importance of oral food intake, and about the dysphagia pyramid in Japan. On next blog, she will talk about progress of the dysphagia diet. Please stay tuned!
Did you find this blog interesting?
Please share it with your friends in the food service industry.
We regularly update the blog about the food culture of Japan, where TREHA® was discovered for culinary applications.
Click here and send us a message to subscribe.
Or hit us up on Instagram @trehalose_sensei!